
Capsular Contracture Around A Silicone Implant
Breast augmentation with silicone implants is still the “gold standard” for breast augmentation and the most popular aesthetic breast surgery procedure. According to 2019 Plastic Surgery Statistics released by the American Society of Plastic Surgeons (ASPS), 287,085 people underwent breast augmentation surgery with silicone implants in a year. The most common late complication of this surgical procedure is “capsular contracture” that requires an additional surgical intervention.
What is Capsular Contracture?
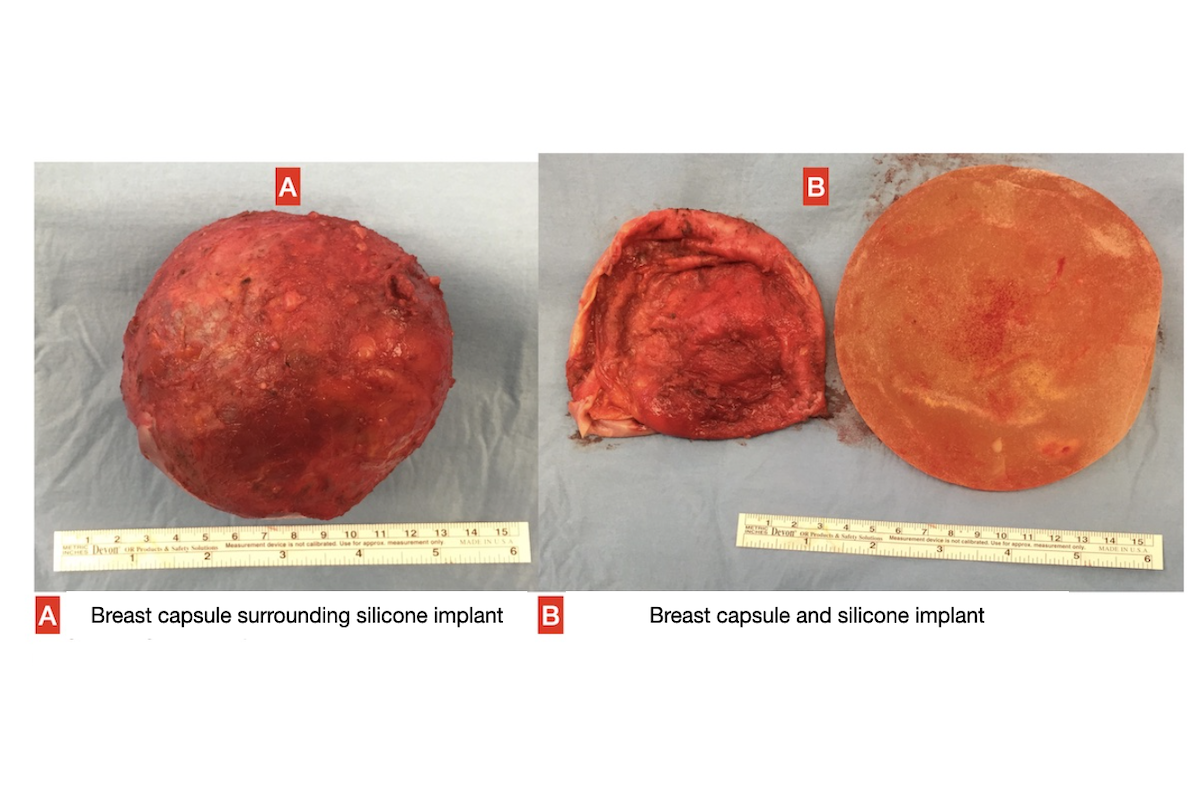
When any foreign substance settles in the human body, the immune system goes into action and surrounds it in a sheath synthesized by connective tissue cells, creating a barrier between the foreign substance and the body. Around silicone implants used in breast augmentation surgeries, all patients develop an “envelope, i.e. sheath,” known as a “capsule” that consists of myofibril fibers, collagen fibers, and connective tissue cells (fibroblast and myofibroblast).
In fact, this capsule has another function, which is to surround the implant, preventing it from slipping and sliding. Since the capsule formed is usually thin and flexible, it does not cause any discomfort to the patients and causes no problem. However, for some reasons, this capsular tissue formed around the silicone implant becomes thicker and harder than normal in some patients, contracting like a ball, tightening the silicone implant, and deforming the breast. The complication is called “capsular contracture”.
What Are The Causes of Capsular Contracture?
Many scientific studies on this subject conducted over the years have suggested that more than one factor contribute to the formation of capsular contracture, and that a “pathological foreign body reaction” develops basically as a result of low-intensity but continuous stimulation of immune system cells surrounding the implant. Factors believed to lead capsular contracture:
Genetic Predisposition: Some people react more strongly to foreign bodies, which may result in more connective tissue synthesis. This process is similar to the poor wound healing called “hypertrophic scar” or “keloid” that occurs as a result of excessive connective tissue synthesis observed after skin incisions in some patients.
For this reason, it can be said that those with autoimmune diseases, an extremely allergic structure, or an excessive wound healing response causing keloid etc., are at a slightly higher risk of capsular contracture. However, it is impossible to know who carries such a genetic risk.
Low Grade Bacterial Infection: Some studies have detected a biofilm layer containing various microorganisms around the silicone implant. Studies have revealed that bacteria settled in the patient’s milk ducts or skin, as well as externally transmitted microorganisms, cause capsule contracture when a silicone implant is placed.
Microbes can be transported to the capsular tissue surrounding the implant via blood when there is a common infectious agent in the blood due to an infection in another part of the body.
Leakage of Silicone Gel into the Environment: The majority of silicone implants used today contain softer silicone gel inside their silicone sleeves. If this silicone gel leaks out of the silicone sleeve or leaks into the environment due to the impairment of the silicone sleeve’s integrity, it causes a severe foreign body reaction in the capsular tissue, resulting in as capsule contracture. It is also likely to cause enlargement of regional lymph nodes in the armpit or rib cage.
Accumulation of Blood Clots or Tissue Fluid Around the Implant: If the blood clots that form around the silicone implant after surgery are not discharged through drains or are not completely absorbed by the body, they can function as a breeding ground for bacteria, increasing the risk of capsular contracture.
Radiotherapy: Capsule contracture is much more likely to develop around silicone implants placed in areas that have been subjected to radiotherapy due to breast cancer.
Placing A Larger-than-Normal Implant: Some people believe that using large implants that create excessive tension around the implant increases the risk of capsular contracture. Therefore, it would be appropriate to place a normal volume implant first, and then replace it with a larger implant after the tissues have loosened after a few years.
Trauma: Capsular contracture can also occur as a result of trauma to the breast in the postoperative period.
Smoking: According to some sources, smokers experience poor connective tissue synthesis and worse wound healing process, and they are at a higher risk of developing capsular contracture.
When Does Capsular Contracture Develop?
The development of capsular contracture is a slow but progressive process. In 75% of cases, capsular contracture develops within the first two years after surgery, while the wound healing process continues. However, capsular contracture may also develop in later periods of life due to a variety of factors such as implant rupture.
What Is The Incidence Rate Of Capsule Contracture?
Although different rates are reported in different study groups, the mean incidence of capsular contracture ranges from 8% to 10%.
How Can I Know If Capsule Contracture Has Developed? What Are Its Symptoms?
- Tingling can be felt around the implant, and there may be some redness in the breast.
- Various degrees of pain ranging from local tenderness to severe pain can be felt in the breast.
- The thickened capsular tissue around the implant causes stiffness and limitation of movement that can be felt when the breast is touched. When a normal breast is touched, the implant is felt soft and mobile.
- When the breast is viewed from the outside, deformity and asymmetry can be seen. As the capsular tissue gradually squeezes the surrounding silicone implant, various degrees of deformation develop in the breast. The implant remains above its normal position and becomes stiff and immobile.
What Are the Grades of Capsular Contracture?
Grade 1: The breast is soft and looks normal, and there is no symptom or complaint.
Grade 2: When viewed from the outside, there is no deformation in the breast, but when the breast is touched, stiffness is felt around the implant.
Grade 3: When viewed from the outside, the breast looks deformed, and when touched, it is felt abnormal and hard. There is not significant pain.
Grade 4: The breast has been noticeably deformed and hardened. When touched, the breast is felt stiff and immobile, and causes tenderness and pain
How Is A Capsule Contracture Diagnosed?
MRI (Magnetic Resonance Imaging) is the most reliable diagnostic test in patients who present with the aforementioned clinical symptoms and complaints. It enables the physician to review the integrity of the silicone implant, the structure of the capsular tissue around the implant and the breast tissue itself.
Ultrasonographic examination also gives an idea, but the doctor who performs it must be sufficiently experienced. In order to detect complications that may occur in the late period, an MRI examination is recommended three years after silicone implant surgery and then every two years after that.
Can Capsule Contracture Develop In Both Breasts?
Capsule contracture does not always develop equally in both breasts. In some cases, it is only seen in one breast, but in the majority of cases, it is seen in both breasts, although more prominently on one side.
What Are the Surgical Treatment Procedures For Capsular Contracture?
There are some surgical procedures performed to treat grade-3 and grade-4 capsule contracture in particular.
Removing A Silicone Implant Without Replacing It With Another One: This is the most effective treatment procedure for capsular contracture because when the silicone implant, as a foreign body, and capsular tissue are removed, both the antigenic stimulus and other risk factors are eliminated. In such a case, the breast skin tissue enlarged by the implant will look emptied and drooping, but a breast lift operation can performed in the same session to obtain a smaller but more aesthetic appearance.
In practice, this is not the most preferred procedure. It is typically used as a last resort after other treatment options have failed and the problem has reoccurred. In selected cases, breast augmentation can be repeated using the patient’s own tissues instead of silicone implants
Open Capsulotomy: The silicone implant is accessed through an incision made on the surgical scar that has been left by the previous operation, the implant is removed, the pouch is cleaned, and the capsule surface is expanded again by making incisions in the horizontal and vertical planes from the inside of the capsular tissue that looks like a dome, but the capsular tissue is left in place. The procedure is terminated by placing the new silicone implants. Although this is a faster and easier procedure in practice, it is not preferred today due to the high recurrence rate of capsular contracture.
Capsulectomy: It is a surgical procedure intended for partial or complete removal of the capsular tissue surrounding the silicone implant. The removal of the biofilm layer rich in bacteria, silicone fragments, calcification foci, and capsular tissue containing myofibroblasts, which actively takes part in contracture, plays a very effective role in the treatment.
Capsulectomy is a surgical procedure that requires experience and carries some complication risks. The answers to the questions of whether a capsulectomy is required and, if so, how to perform a capsulectomy operation may differ from patient to patient and depend on the experience of the plastic surgeon. It is useful to send the removed capsular tissue for routine pathological examination in order to investigate whether tumor cells exist in these tissues, and confirm that the tissue is entirely composed of capsular tissue.
Repositioning the Implant (Creating a New Pouch): Changing the location of the pocket where the silicone implant has been placed, by creating a new pouch and placing the new silicone implants in this new pouch is an important method in the treatment of capsular contracture.
Especially in the treatment of capsular contracture that occurs around the implant placed in a pouch created in the subglandular plane (supramuscular-submammary plane), the use a newly created pouch in a subpectoral (submuscular) plane is an extremely effective method. If the implant is in a in a subpectoral (submuscular) pouch, a new supramuscular pouch can be created. However, this change may not be possible in cases where the muscle and breast tissue has become tin after prolonged exposure to pressure. In such a case, the implant is removed, the anterior surface of the capsular tissue is positioned on the lower surface and a new pouch is created between the anterior surface and the chest muscle.
Acellular Dermal Matrix: The dermis part of human, pig or bovine skin is purified from cells by being subjected to some processes and is offered for use in the form of sheets. The rate of capsular contracture is claimed to be significantly reduced when this material partially or completely wraps the silicone implant, preventing direct contact between the silicone implant and the surrounding tissues. It is used to treat recurrent capsular contractures or submuscular capsular contractures, particularly in areas that have been subjected to radiotherapy.
Silicone Implant Replacement: During the capsectomy and pouch repositioning procedures, which are the most common procedures performed in the surgical treatment of capsular contracture, the removed old silicone implants are replaced with new ones. If the removed implants are larger than the pouch sizes, smaller implants suitable for the newly created pouches are preferred.
What Are The Non-Surgical Treatment Procedures For Capsular Contracture?
Closed Capsulotomy: It is based on the principle of applying external force to burst and tear the capsular tissue surrounding the silicone implant. It is no longer performed due to its high recurrence rates and some complications.
Drug Therapy: There are studies reporting that some drugs intended to suppress inflammation that is a process playing a critical role in the formation of capsular contracture are beneficial. Among these, the most prominent ones are some drugs known as leukotriene antagonists, which are used to treat diseases such as allergic asthma or allergic rhinitis. It is reported that they can be used as a precaution, particularly in cases at the initial stages or in cases where capsular contracture has been surgically treated before.
Ultrasonic Wave Therapy: There are studies reporting that applying an externally controlled ultrasonic wave to the capsular tissue through instruments like the Aspen Harmonizer stimulates the formation of healthy collagen and softens the capsular tissue.
How Should The Surface Of The Silicone Implant To Be Newly Placed Be Like?
Textured-surface implants are claimed to cause less capsular contracture than smooth-surface implants. However, there are also studies suggesting that implant surface properties have no significant effect on the formation of capsular contracture.
In recent years, there has been an increase in the tendency to use smooth-surface implants, as it has been reported that anaplastic large-cell lymphoma (ALCL) around the implant are more common in cases where textured-surface implants are used. There is no consensus on this matter. In my practice, I use smooth-surface implants for all my patients.
Does Capsular Contracture Recur After Treatment?
Even if the necessary surgical procedures are fully performed in the treatment of capsular contracture, there is still a risk of recurrence, except in cases where silicone implants are removed and without placing new ones. If there is an obvious cause of capsular contracture, such as a ruptured implant, the capsular contracture is less likely to recur when this cause is eliminated.
Does Massage Prevent the Development of Capsular Contracture?
There is a procedure intended to stretch and loosen the capsular tissue by massaging the silicone implants in the weeks following the surgery. However, the benefit of massage is debatable. Massage can be harmful rather than beneficial. This matter should be consulted with the plastic surgeon who has performed the surgery. I do not recommend massage to my patients.
Is Capsular Tissue Harmful?
The capsular tissue itself is not harmful, so it does not require immediate treatment. However, the signs and symptoms of capsular contracture are similar to those of “Anaplastic Large Cell Lymphoma” that develops around the implant. Therefore, a very thorough evaluation should be made during the diagnosis and treatment phases.
Magnetic resonance imaging (MRI) and ultrasonographic techniques should be used to assess the breast. The possibility of a mass should be investigated, and if fluid accumulation is detected around the implant, this fluid should be reviewed with cytological examination. When the capsular tissue is surgically removed, it should be sent for pathological examination. The treatment of capsule contracture does not require removal of the entire capsule, but in cases of anaplastic large cell lymphoma, the tissue surrounding the implant should be completely removed in a more radical way.
My Dos And Don’ts For First Breast Augmentation Operations, As Precautions Against Capsular Contracture Development
In my practice, among those whom I previously treated with breast augmentation surgery, no one has returned to me with a capsule contracture severe enough to necessitate surgical intervention. I can list the factors that have an effect on this result as follows:
- I do not apply silicone implants to patients who have received radiotherapy for breast cancer.
- I prefer a silicone implant brand that has been in use for a long time and has proven to be of high quality. I don’t try any newly launched brands.
- I place the silicone implant through an incision made on the inframammary fold, and avoid as much as possible cutting the milk ducts.
- In the vast majority of cases, I prepare a pouch in a subpectoral plan (also known as submuscular or dual plan) and place the implant in it.
- During surgical operations, I take serious precautions to avoid infection.
- I manage bleeding very carefully.
- I definitely use drains to discharge the blood and tissue fluids that form after surgery, and I don’t remove the drains until the amount of drainage is reduced enough.
- I don’t attempt to place a large implant that would impel the dimensions of the pouch I prepared.
- I don’t recommend massage.
- I ask my patient to wear a special corset for the first 6 postoperative weeks.
Which Treatment Option Is the Best Fit for You?
The plastic surgeon evaluates each patient who presents with the complaint of capsular contracture to determine possible treatment options. The patient and her physician discuss the advantages and disadvantages of each procedure and then make a decision. Plastic surgeons may differ from each other in terms of treatment approaches and preferences, and this is natural.




